New Delhi: Pawan Kumar arrived at the DOTS centre in the government-run Deen Dayal Upadhyay Hospital at 7:30 am, half an hour before it opens. He was with his sister, Shanti, and their mother, but in spite of the family’s early start, there were already 15 patients ahead of Pawan, waiting for TB treatment. Shanti, a cook, had permission from her employer to arrive late, but Pawan’s mother, a domestic worker, did not. She had to take the entire day off, losing a full day’s wages.
A few days ago, when Pawan first visited the centre by himself, he had left with a TB diagnosis, a prescription and medication but no clarity about his condition. “I didn’t do much schooling, so I could not understand what the doctor said. But this time, my sister, who is educated, has come to help me understand,” Pawan said matter-of-factly.
In late March, when The Migration Story met Pawan, his eyes were sunken and his frame stripped of fat. His struggle with TB had taken a toll: he looked decades older than he was.
“I have had a persistent cough since January. I used to work as a labourer but due to prolonged weakness and aching feet, I stopped working six months ago,” said Pawan, 28, whose family hails from Uttar Pradesh. His parents and older brother moved to the capital in 1993 seeking a better livelihood.
The family now lives in a tiny room in Pili Kothi, a slum in the Hari Nagar residential area. The room has a single bed against the back wall and around two arm-lengths of space to the door. Pawan had recently lost his appetite, but couldn’t understand why — until his diagnosis a few days ago. Still, he remains hopeful, “It is difficult, but times are different now,” he said, sitting down for lunch at home. “I am taking medicine, and I know I will get better.”
Due to the socio-economic hardships they face, migrants are extremely vulnerable to infectious diseases, especially tuberculosis, and are considered a high-risk population in the National Strategic Plan to End TB. The lack of inclusive urban planning has forced them to live in congested and overcrowded slums, significantly increasing their chances of getting the disease.
Like Pawan, most of Pili Kothi’s nearly 2,000 residents are migrants who came to the capital seeking better prospects, said Ashok Kumar, who heads the Pili Kothi Jhuggi Association, a local group that represents the slum’s residents. Their homes are one-room structures shared by at least four people, and the alleys here are so narrow, you have to tuck your arms inward just to walk through them. Many dwellings are just two feet from each other, and most hardly ever get direct sunlight or breeze.
Ashok, 54, a migrant from Bihar, observed that TB’s spread in his community was a direct consequence of the lack of space. “When all you have is 10 gaj [90 square feet] and in it you have to live and cook with your family, you have no alternative but to share space, even if someone in the family is infected [with TB]. You don’t have the money to make any other arrangement,” he told The Migration Story on the phone.
Health experts say that high-density housing and environmental factors, such as light, air and space, play a significant role in the spread of air-borne TB, particularly in urban slums where homes and workplaces are small and overcrowded. Though recent government programmes have reportedly improved TB’s early detection, studies say that improving indoor ventilation is as necessary as medical intervention and an important pre-emptive step to end TB globally.
THE DESIGN PROBLEM OF INFORMAL SETTLEMENTS
India has not been able to meet its pledge of eliminating TB by 2025, accounting for 25% of global tuberculosis cases in 2024, making it the top-ranked country for TB incidence, according to the 2025 Global Tuberculosis Report. In 2023, there were over 3.23 lakh deaths in India due to TB; in other words, 37 Indians died every hour.
Of the different kinds of Mycobacterium tuberculosis, pulmonary TB attacks the lungs and is contagious. Tuberculosis bacilli are present in phlegm and when patients cough, infectious droplets with the bacilli are released into the surroundings. These bacilli remain viable for a long time, and in overcrowded informal settlements like Pili Kothi where homes get little sunlight and are poorly ventilated, the chances of the disease spreading are high.
In fact, public health researchers have observed a 97% drop in new TB cases in adequately ventilated indoor spaces. Doctors recommend isolation of the TB patient, wearing masks and maintaining social distance until a TB patient tests negative.
“If you have a big, airy house with a lot of windows and doors, the spread will be very limited, but if five to ten people are sharing a single room with no ventilation, the spread will be much higher,” said Dr. Harprit Singh, a District Tuberculosis Officer, at the DOTS centre, which treats TB patients for free under the globally recognised DOTS framework.
There is a design problem in urban informal settlements, Dr. Singh observed, adding that screening for TB is the only defensive tool against the disease, given the architecture of slums and the challenges of relocating slum-dwellers.
The government has said that its treatment protocols under the National Strategic Plan (NSP) to End Tuberculosis in India (2020-25) are much improved now, with increased screening for TB, community involvement and local health services. But the environment in urban slums — light, air and space — impacts both the transmission of and recovery from tuberculosis, said Dr. Singh.
To combat this, he said that the overall strategy must go beyond the individual. “Our [the government’s] approach relies on early diagnosis and awareness, but we cannot stop at the patient: we must screen every household member. When a patient lives with four or five others in close quarters, the risk is extreme,” he explained.
This risk is visible in the home of Ranjit Lal, 40, a migrant from Bihar who lives just a few lanes away from Pawan. Two years ago, Ranjit’s wife, Anita Devi, was diagnosed with pulmonary TB. Though she completed her six-month DOTS regimen, she suffered from the disease for an entire year. The family went for a follow-up screening a few months after her recovery only to find out their daughter Sanjana, 19, also had TB.
Ranjit said that while he and his younger son, Hritik, can escape the stifling summer heat by sleeping on the roof of their home, the women stay inside the room because of cultural norms and concerns around safety. Thus, the women end up spending more time indoors than men, where the air is stagnant and could have a higher concentration of airborne bacteria.
Two months after Sanjana was diagnosed, healthcare workers with the National Tuberculosis Elimination Programme (NTEP), the central initiative that executes the National Strategic Plan (NSP) to End Tuberculosis, insisted the family be tested again.
But Ranjit was sceptical. “I thought testing again was futile. I had no symptoms, no cough, no mucus, but they insisted,” he said in the small room where he was isolated with Sanjana.
Ranjit’s test results came back positive — he had been in the “latent phase” of the disease. “When a germ enters the body, it takes time to proliferate before it produces symptoms,” Dr. Singh explained. “This incubation period or latent phase can last from a few days to several weeks and sometimes longer. The bacteria are there, even if the symptoms are not.”
TUBERCULOSIS TREATMENT IN URBAN SLUMS
In December 2024, the Ministry of Health and Family Welfare launched the 100-Day TB Mukt Bharat Abhiyaan, an intensive TB elimination drive in 347 high-priority districts across the country. Till March 2026, the government said that it had screened over 20 crore vulnerable people, including 28 lakh TB patients.
Medical teams visiting urban slums like Pili Kothi use portable handheld x-ray machines and other rapid and sensitive diagnostic tools, doing systematic screenings there. Healthcare workers use methods like nukkad natak (street theatre) and magic shows to make health information more accessible to the migrants living in these settlements.
But the government’s health camps often fall short, said Ashok. “They come once a year for the sake of it. When a patient is tested in a hospital, they take x-rays and do ultrasounds, but none of that happens in these camps. The explanations that doctors give are poor, and people quickly lose the motivation to follow through,” he said.
Sometimes, survival also gets in the way of treatment for migrants. “When residents are told to open windows to prevent the spread of TB, they tell us they have to keep them shut to avoid getting dengue or malaria,” said Dr. Ramya Ananthakrishnan, the director of REACH, a nonprofit working on tuberculosis with communities in six states.
Rajni Kumari, who moved to New Delhi from Bihar after her marriage, was seeking treatment for TB at the DOTS centre for the second time. “I was healthy in Bihar — I did not even know what TB was — but here I keep coming to the hospital and taking medicines,” said Kumari, whose husband is a daily-wage labourer.
While TB is often linked to poverty, it is not strictly a “poor man’s disease”, said Dr. Ananthakrishnan, and anyone can get it. “TB is linked to poverty because poverty is associated with overcrowding and a lack of ventilation. It’s not a ‘poor man’s disease’ by nature but by circumstance,” she observed.
“Their lives may be inadequate, their needs for basic things like food or support or infrastructure may not be properly met. They may not be eating well, be undernourished or have immunosuppressive diseases like HIV or cancer.”
The architectural problems of the slums are also exacerbated by the changing climate. Dr. Singh observed that annual data for TB cases showed a distinct inverted V with the change in seasons. The numbers were low in the winters, peaked in the summers, especially in the sweltering months of May and June, and dipped again after the monsoon.
“Heat and humidity play a significant role as they enhance the bacteria’s ability to spread,” he explained. In the stagnant, unventilated interiors of Pili Kothi, high humidity in the summer provides the ideal conditions for tuberculosis bacilli to stay viable and circulate.
Apart from this, the ratio of diagnosed tuberculosis cases in India among men versus women is approximately 2:1. However, this does not necessarily mean that women get TB less often. Rather, it reflects the fact that women often face barriers while accessing TB treatment. When they do, it can have repercussions, such as domestic violence and desertion, according to a 2025 academic paper on women and tuberculosis care in India.
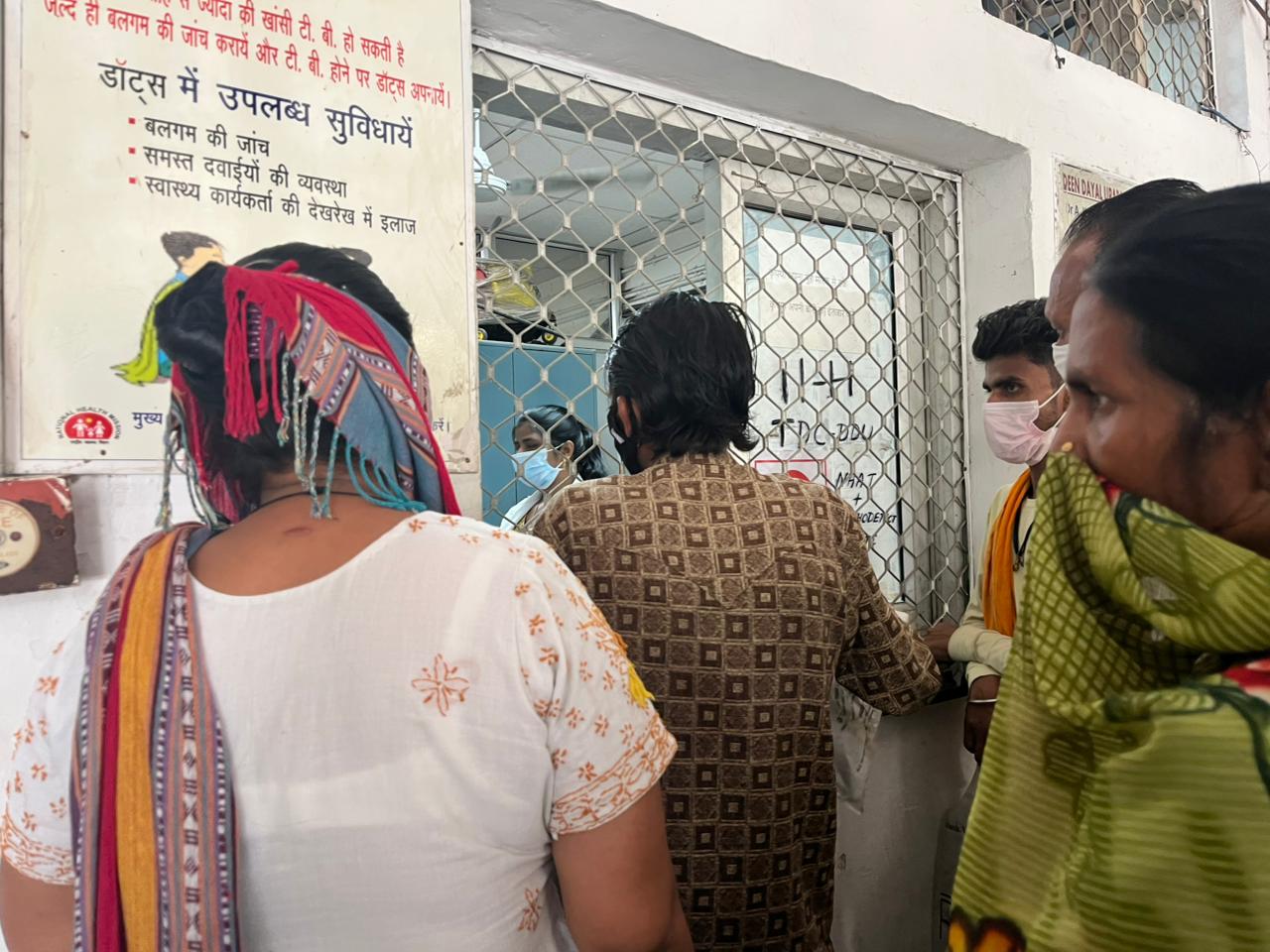
Doctors often don’t have time to explain diagnoses to TB patients, so Pawan Kumar went to the DOTS centre with his sister (left, in white), who is more educated than him, and his mother (right). Swati Thapa/The Migration Story
Like Pawan, Rajni was also waiting in line at the DOTS centre, but she didn’t come with a supportive family member. Her immediate family is still in Bihar, and her husband, who had accompanied her, often fights with her because she has TB.
“My husband says I will die. He drinks and when he is drunk, he fights with me about how I keep getting TB and complains about it to everyone,” Rajni said while her husband was away handling payments.
Rajni, a homemaker, drops her children off at school every day, but on days she has to visit the DOTS centre, the children are forced to skip school. Her worries don’t end with her appointment, however; she is often afraid of what awaits her at home when her husband returns from work.
“He cannot fight me here because he knows that people would intervene, but as soon as we return home, he starts fighting with me and doesn’t even spare our children,” Rajni added.
LACK OF SUNLIGHT IN SLUMS, RESETTLEMENT COLONIES
The risk of tuberculosis spreading quickly isn’t restricted to slums, however. Slum rehabilitation programmes often relocate slum-dwellers to resettlement colonies where the ventilation is poor and sunlight, limited. A 2020 academic study found that TB prevalence was as high as 10% in crowded, poorly ventilated buildings in such colonies in Mumbai, but dropped to 1% in buildings that had better ventilation.
This health risk, the authors said, arises due to relaxed development rules that prioritise density over livability. Sunlight is a natural disinfectant, and ventilation lowers airborne germs. But because there are a high number of units in a single building and often, very little space between the buildings, residents can’t even open their windows sometimes. They end up living in dark spaces where the air is stagnant, creating what the authors call “pressure-cooker” conditions that heighten the risk of airborne TB.
Dr. Vaishali Venu, Director of Health at Doctors For You, a Mumbai-based organisation that was part of the study, pointed out the irony inherent in slum rehabilitation programmes — old slums are cleared for redevelopment and their inhabitants are pushed into even denser housing on the city’s peripheries.
“This modern urban living leaves the vulnerable with nowhere to go when the very walls of their homes are the source of their sickness.” said Dr. Venu. According to 2025 data from UN Habitat, approximately 41.4% of India’s urban population lives in slums. So, the stories of Pili Kothi’s residents and their struggles with tuberculosis aren’t isolated ones — they could likely be found in slums in India’s other mega-cities too.
FEAR, DISCRIMINATION AND AN INDIFFERENT PUBLIC HEALTH SYSTEM
In government-run DOTS centres, patients don’t often get individual attention and end up with little information about their condition. “Unfortunately, in this government setup, we don’t have the time to explain things in detail,” said Dr. Singh. The centre is stretched thin, with only four doctors handling the entire district’s — and in this case, all of New Delhi’s — TB burden, he added.
This manpower crisis could have been the reason that Pappu Kumar, 27, a migrant from Bihar, had to navigate his recovery from TB in fear. The doctor at the DOTS centre didn’t explain to him that a patient typically becomes non-infective after two weeks of consistent medication. So, Pappu ended up spending six months sleeping on the cold floor outside his home, away from his family.
“I have not held my children in my arms for six months now,” he said, with a lump in this throat. “They come running to me and want me to hold them, but it’s hard for me to explain to them why I can’t.”
Ashok also explained why people often postpone visiting government hospitals, even though they have symptoms of the disease. “Many do not go to government hospitals at first because they are not treated fairly and face [caste] discrimination,” he said.
The fear of homelessness also makes many slum-dwellers hesitant to come forward and report symptoms. Dr. Ananthakrishnan added that patients often refuse to have their roommates screened because the mere mention of TB can lead to immediate eviction by landlords.
“An educated person who understands the disease will go and get further treatment on time, but many people here [in Pili Kothi] are illiterate,” said Ashok. “They earn daily, they eat daily, and when survival depends on today’s wages, navigating hospital formalities gets pushed aside or simply forgotten.”
Swati Thapa is a freelance journalist from Uttarakhand, who covers gender, environment, health and other topics.